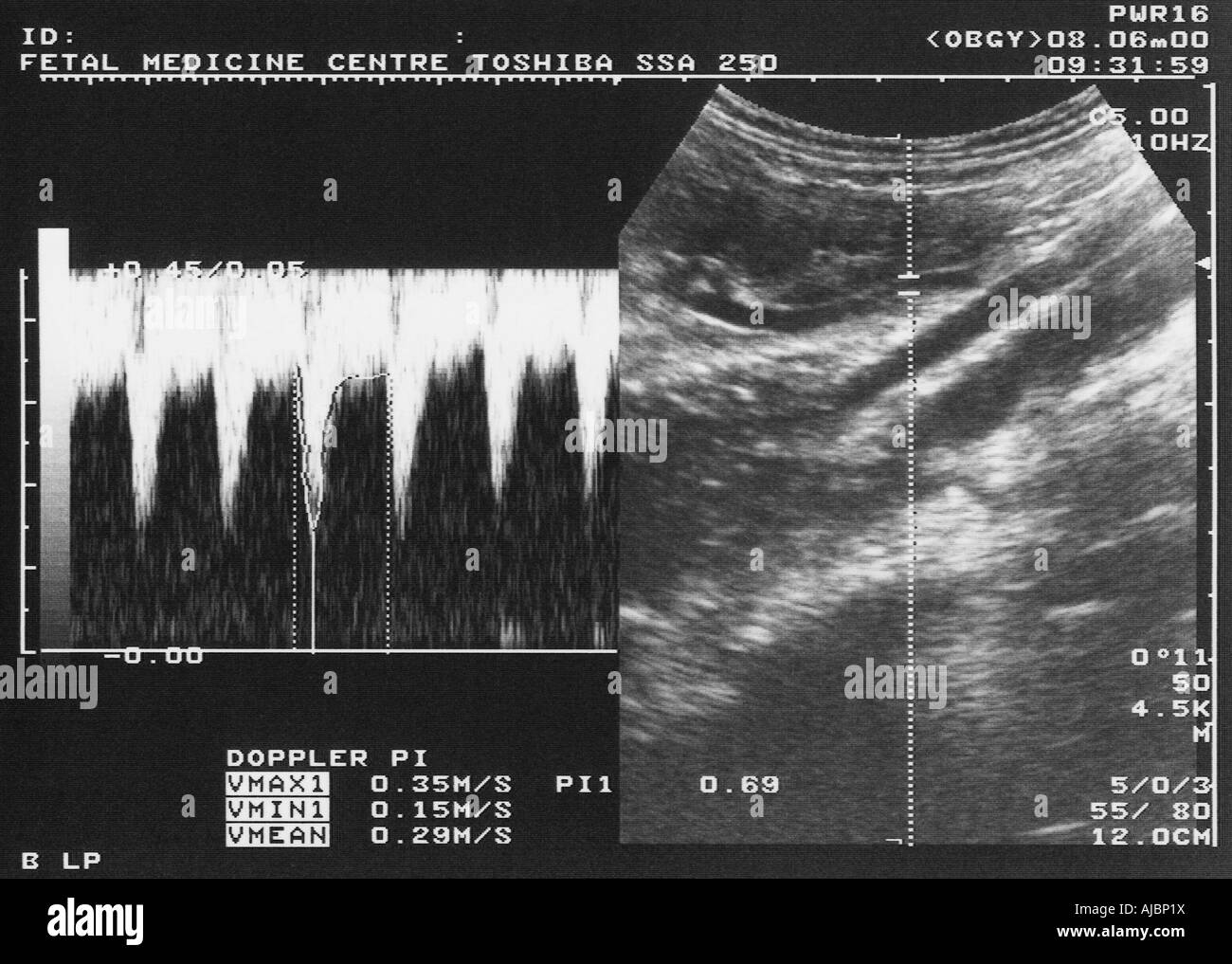
A Doppler ultrasound scan uses high frequency sound waves to create images. These images show the blood flow going between the mother and baby and gives a good idea of how well the placenta has developed and will perform during the remainder of the pregnancy. The head-to-abdomen circumference ratio, as measured by ultrasound, differentiates between symmetric and asymmetric fetal growth restriction. Symmetric fetal growth restriction tends to occur before 28 weeks gestation. The head-to-abdomen circumference ratio is normal, but the absolute values of biparietal head circumference and abdominal circumference are low. These cases tend to be caused by congenital anomalies or TORCH infections. Asymmetric fetal growth restriction tends to occur after 28 weeks gestation and is marked by the fetal head growing at its usual rate, but the body failing to grow. The head-to-abdomen circumference ratio is high. The most common cause of fetal growth restriction (also called intrauterine growth restriction) is placental insufficiency where the placenta cannot deliver enough blood and nutrients to the growing fetus. This usually results in the asymmetric type of FGR since the fetus tries to spare blood to be used by the most important organs (e.g. brain and heart). For this reason in advanced cases of placental insufficiency FGR, the head size is usually spared whereas the abdominal circumference is small for gestation. However, the fetus can only compensate in this manner for a limited time-period after which fetal heart failure ensues and the fetus's situation becomes critical. Placental insufficiency can be predicted by uterine artery Doppler measurements in the first or second trimester. Once FGR is present, fetal Dopplers (e.g umbilical artery, middle cerebral artery, and ductus venosus Doppler) are very helpful in assessing fetal health and deciding on the best time for delivery.
{kind=link}